Evaluation of myxomatous mitral valve disease in dogs
Thuy Hoang Nguyen1 Kinh Van La1 Yen Hai Vu1 Quynh Ngoc Nhu Nguyen1 Loan Vu Thuy Hong Nguyen1*
- Faculty of Veterinary Medicine and Animal Science, HUTECH University, Binh Thanh District, Ho Chi Minh City 717000, Vietnam
Article Information
- Date Received: 21/01/2026
- Date Revised: 10/04/2026
- Date Accepted: 26/04/2026
- Date Published Online: 27/04/2026
Copyright: © 2026 The Authors. Published by MARCIAS AUSTRALIA, 32 Champion Drive, Rosslea, Queensland 4812, Australia. This is an open access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Citation: Nguyen TH, La KV, Vu YH, Nguyen QNN, Nguyen LVTH (2026). Evaluation of myxomatous mitral valve disease in dogs. Aust J Agric Vet Anim Sci (AJAVAS), 2(1), 100013
https://doi.org/10.64902/ajavas.2026.100013
Abstract
This study aimed to evaluate the prevalence, clinical characteristics, diagnostic indicators, and treatment outcomes of myxomatous mitral valve disease (MMVD) in dogs in Vietnam at Procare Veterinary Hospital. From October 2024 to October 2025, a total of 3,840 dogs presenting with respiratory signs or undergoing health screening were examined. Dogs suspected of cardiac disease were further evaluated using thoracic radiography, echocardiography, and N-terminal pro-B-type natriuretic peptide (NT-proBNP) quantification. A total of 232/3,840 dogs (6.04%) were suspected of cardiac disease, of which 84 dogs (36.21%) were confirmed to have MMVD, accounting for 2.19% of all examined dogs. The most common clinical signs were dyspnea/pulmonary edema and cough, with increasing frequency from stage B1 to C. Cardiac murmur intensity increased with disease progression, with most dogs in stages B2 and C having murmurs ≥ grade III/VI. Echocardiographic variables of left-sided volume overload, including vertebral heart size (VHS), left atrium to aorta ratio (LA/Ao), left ventricular internal diameter in diastole (LVIDd), and systole (LVIDs), increased significantly across stages (p < 0.001), whereas fractional shortening showed no significant change (p = 0.575). NT-proBNP concentrations increased from 500 pg/mL (B1) to 953.8 ± 294.0 pg/mL (B2) and 2,131.8 ± 354.4 pg/mL (C). Treatment outcomes were favourable in stage B2 (98.18%) but markedly lower in stage C (43.48%). These findings highlight the importance of combined clinical, imaging, and biomarker evaluation for accurate staging, early detection, and improved management of MMVD in dogs
Keywords
Myxomatous mitral valve disease; dogs; echocardiography; NT-proBNP.
Highlights
- Myxomatous mitral valve disease affected 2.19% of examined dogs; respiratory signs increased with disease stage.
- Echocardiographic variables of left-sided volume overload and NT-proBNP increased significantly from stage B1
to C. - Early-stage treatment was highly successful, but outcomes declined markedly in stage C.
1.0 Introduction
Myxomatous mitral valve disease (MMVD) is one of the most common acquired cardiac diseases in dogs, particularly prevalent in small breeds and geriatric animals. The disease is characterized by progressive degeneration of the mitral valve leaflets, leading to incomplete valve closure, mitral regurgitation, left atrial enlargement, and chronic volume overload, which may eventually progress to congestive heart failure if not diagnosed and managed appropriately (Keene et al., 2019; Häggström et al., 2008).
In Vietnam, particularly in Ho Chi Minh City, published data on MMVD remain limited. Previous studies in small animal practice have primarily focused on clinical presentation and basic diagnostic findings, with reported prevalence ranging from approximately 1.5% to 3% among examined dog populations. However, these studies have not comprehensively evaluated the combined use of echocardiography, thoracic radiography, and cardiac biomarkers such as N-terminal pro-B-type natriuretic peptide (NT-proBNP) in disease staging and monitoring. Moreover, detailed analyses of treatment outcomes across different ACVIM stages are still lacking in the local context.
Therefore, this study aimed to evaluate the prevalence, clinical characteristics, diagnostic indicators, and treatment outcomes of MMVD in dogs at a veterinary hospital in Vietnam. By integrating clinical examination, imaging modalities, and biomarker assessment, this study seeks to provide a more comprehensive understanding of MMVD and to address existing gaps in diagnosis and disease management under practical veterinary conditions.
2.0 Materials and methods
2.1. Study site, animals, housing, and experimental design
The study was conducted from October 2024 to October 2025 at Procare Veterinary Hospital, Phu Nhuan District, Ho Chi Minh City. Dogs included in the study were those presenting with clinical signs such as cough, dyspnea, exercise intolerance, fatigue, or syncope, as well as dogs without clinical signs that were brought for routine annual health screening or pre-anaesthetic examination.
2.2. Data collection
2.2.1. Clinical examination and classification of dogs suspected of MMVD – Cardiovascular clinical Examination
After collecting a complete history from the owner, dogs underwent a general clinical examination with particular focus on the cardiovascular system. Cardiac auscultation was performed using a stethoscope to detect systolic murmurs, a characteristic sign of myxomatous mitral valve disease, most clearly heard at the 4th–6th intercostal spaces (Turgut et al., 2019). Murmur intensity was graded from I to VI according to severity (Pedersen et al., 1999). Heart rate was recorded, with normal physiological values ranging from 60 to 140 beats per minute; in dogs with MMVD, heart rate may increase due to compensatory mechanisms. Peripheral pulse was assessed to reflect circulatory status; weak or irregular pulses may be associated with cardiac dysfunction. Resting respiratory rate was measured, with normal values of 18–34 breaths per minute; a rate above 30 breaths per minute often suggests congestive heart failure or pulmonary oedema (Goutal et al., 2010).
2.2.2 Procedures for Assessing Paraclinical Parameters in MMVD
Paraclinical evaluation followed a standardized protocol including thoracic radiography, echocardiography, and NT-proBNP testing.
Thoracic radiography:
Thoracic radiography was performed in dogs presenting respiratory signs or when cardiac disease was suspected based on clinical examination. Dogs were positioned in right lateral and ventrodorsal recumbency with gentle restraint. Images were obtained using a digital X-ray system and analyzed for cardiac size and shape, left atrial and ventricular enlargement, and signs of pulmonary edema or pleural effusion. The vertebral heart size (VHS) was calculated according to Buchanan and Bücheler, with normal values ranging from 8.7 to 10.5 vertebrae (Buchanan & Bücheler, 1995).
Echocardiographic evaluation:
Echocardiography was performed in all dogs suspected of MMVD based on clinical or radiographic findings. Dogs were positioned in lateral recumbency, and transthoracic echocardiography was conducted using two-dimensional (2D), M-mode, and color Doppler imaging. Two-dimensional imaging was used to evaluate mitral valve morphology.
M-mode was used to measure left ventricular internal diameter in diastole (LVIDd) and left ventricular internal diameter in systole (LVIDs). These values were normalized to body weight to obtain LVIDd normalized (LVIDdN) and LVIDs normalized (LVIDsN) according to Cornell et al. (2004). Fractional shortening (FS) was also calculated.
The left atrium to aorta ratio (LA/Ao) was measured to assess left atrial enlargement, with values > 1.6 indicating significant enlargement (Keene et al., 2019). Color Doppler imaging was used to detect and assess mitral regurgitation. Additional parameters included ejection fraction (EF) and E/A ratio for evaluation of systolic and diastolic function (Oyama et al., 2009).
NT-proBNP Testing:
NT-proBNP testing was performed in a subset of dogs with suspected MMVD to support diagnosis and assess disease severity. Blood samples were collected from peripheral veins, processed according to the manufacturer’s instructions, and analyzed using a fluorescence analyzer.
NT-proBNP concentrations < 900 pmol/L were considered within normal limits, whereas values > 1500–1800 pmol/L indicated increased risk of heart failure, and concentrations > 2000 pmol/L were commonly associated with overt congestive heart failure (Oyama et al., 2009).
2.2.3. Classification of dogs with MMVD
Based on clinical findings and results from diagnostic imaging and biomarker analysis, dogs diagnosed with MMVD were classified into stages B1, B2, C, and D according to the criteria established by the American College of Veterinary Internal Medicine (ACVIM) guidelines (Keene et al., 2019).
2.3. Statistical Analysis
Data were collected on an individual basis and analyzed using Excel 2010 and Minitab 17. Quantitative variables were expressed as mean ± standard deviation (SD) for normally distributed data, or as median (minimum–maximum) for non-normally distributed data. Comparisons of means were performed using one-way analysis of variance (ANOVA, F-test) followed by Tukey’s post-hoc test for normally distributed variables. For non-normally distributed data, appropriate non-parametric tests were applied. Percentages were compared using the Chi-square (χ²) test. Differences were considered statistically significant when p ≤ 0.05.
3.0 Results
3.1. Survey of dogs suspected of and diagnosed with MMVD
From October 2024 to October 2025, a total of 3,840 dogs were presented for health screening or examination due to respiratory signs at Procare Veterinary Hospital. Dogs showing clinical signs suggestive of cardiac disease were selected for further evaluation using diagnostic imaging and supportive laboratory tests; the results are presented in Figure 1.
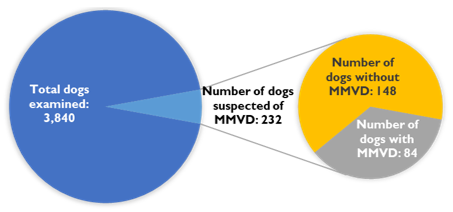
Fig. 1. Number of dogs suspected of MMVD and dogs diagnosed with MMVD at Procare Veterinary Hospital
According to Figure 1, 232/3,840 dogs (6.04%) were suspected of cardiac disease based on clinical signs such as heart murmur, coughing, and reduced exercise tolerance. Echocardiography confirmed MMVD in 84/232 dogs (36.21%), corresponding to 2.19% of all examined dogs.
3.2. Frequency of clinical signs in dogs with MMVD
The frequency of clinical signs in dogs with MMVD is presented in Table 1.
Table 1. Frequency of Clinical Signs in Dogs with MMVD (n = 84)
| Clinical sign | Stage B1 | Stage B2 | Stage C | Total | P-value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | ||
| Tachypnea/ Dyspnea/ Pulmonary oedema | 0 | 0.00 | 55 | 36.67 | 23 | 44.23 | 78 | 37.50 | |
| Cough / Respiratory Inflammation | 0 | 0.00 | 53 | 35.33 | 13 | 25.00 | 66 | 31.73 | |
| Asymptomatic / Decreased appetite | 6 | 100 | 22 | 14.67 | 1 | 1.92 | 29 | 13.94 | 0.000 |
| Reduced exercise tolerance | 0 | 0.00 | 19 | 12.67 | 2 | 3.85 | 21 | 10.10 | |
| Syncope / Transient loss of consciousness | 0 | 0.00 | 1 | 0.66 | 13 | 25.00 | 14 | 6.73 | |
The most common clinical signs were dyspnea/pulmonary oedema (37.50%) and cough/respiratory inflammation (31.73%).
In stage B1, clinical signs were minimal, with most dogs presenting only cardiac murmurs. In stage B2, dyspnea/pulmonary oedema (36.67%), cough (35.33%), and decreased appetite (14.67%) were observed.
In stage C, dyspnea/pulmonary oedema (44.23%), syncope (25.00%), and reduced exercise tolerance were recorded.
3.3. Classification of cardiac murmur intensity by disease stage according to ACVIM
Cardiac murmur intensity increased across disease stages (Table 2).
Table 2. Cardiac murmur intensity by disease stage according to ACVIM
| Heart murmur grade | Stage B1 | Stage B2 | Stage C | Total | P-value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | Number of dogs | Percentage (%) | ||
| 0/VI | 2 | 33.33 | 0 | 0.00 | 0 | 0.00 | 2 | 2.38 | 0.000 |
| I/VI | 3 | 50.00 | 2 | 3.64 | 0 | 0.00 | 5 | 5.95 | |
| II/VI | 1 | 16.67 | 12 | 21.82 | 0 | 0.00 | 13 | 15.48 | |
| III/VI | 0 | 0.00 | 31 | 56.35 | 6 | 26.09 | 37 | 44.05 | |
| IV/VI | 0 | 0.00 | 8 | 14.55 | 12 | 52.17 | 20 | 23.81 | |
| V-VI/VI | 0 | 0.00 | 2 | 3.64 | 5 | 21.74 | 7 | 8.33 | |
| Total | 6 | 100 | 55 | 100 | 23 | 100 | 84 | 100 | |
In stage B1, murmurs were predominantly low grade. In stage B2, grade III/VI murmurs were most frequent (56.35%).
In stage C, murmurs were mainly grade IV/VI (52.17%) and grades V–VI/VI (21.74%), although grade III/VI murmurs were also observed (26.09%).
3.4. Radiographic and echocardiographic indices in dogs at different ACVIM stages
Radiographic and echocardiographic parameters are presented in Table 3 and Figures 2–3.
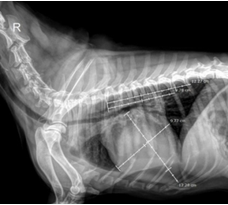
Fig. 2. Measurement of VHS in Dogs with MMVD
The vertebral heart size (VHS) increased significantly from stage B1 to B2 and C (p < 0.001), with mean values of 10.00 ± 0.19, 10.85 ± 0.18, and 11.66 ± 0.32, respectively.
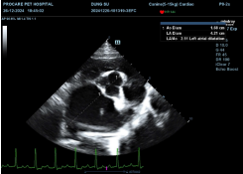
Fig. 3. Measurement of the LA/Ao ratio in dogs with MMVD
The left atrium to aorta ratio (LA/Ao) increased significantly (p < 0.001), from 1.38 ± 0.10 (B1) to 1.76 ± 0.08 (B2) and 2.18 ± 0.17 (C).
Table 3. Radiographic and echocardiographic parameters in dogs with MMVD at different ACVIM stages
| Stage | Statistical parameters | Indices | ||||
|---|---|---|---|---|---|---|
| VHS | LA/Ao | FS | LVIDd | LVIDs | ||
| B1 | n | 6 | 6 | 6 | 6 | 6 |
| Mean | 10.00c | 1.38c | 59.82c | 1.47c | 0.67c | |
| SD | 0.19 | 0.10 | 9.35 | 0.03 | 0.12 | |
| Min | 9.80 | 1.26 | 40.51 | 1.42 | 0.54 | |
| Max | 10.30 | 1.51 | 60.72 | 1.50 | 0.85 | |
| B2 | n | 55 | 55 | 55 | 55 | 55 |
| Mean | 10.85b | 1.76b | 52.03a | 1.75b | 0.81b | |
| SD | 0.18 | 0.08 | 9.47 | 0.03 | 0.10 | |
| Min | 10.60 | 1.62 | 37.26 | 1.70 | 0.65 | |
| Max | 11.20 | 1.91 | 80.35 | 1.84 | 0.99 | |
| C | n | 23 | 23 | 23 | 23 | 23 |
| Mean | 11.66a | 2.18a | 49.70a | 2.03a | 0.99a | |
| SD | 0.32 | 0.17 | 9.90 | 0.06 | 0.09 | |
| Min | 11.00 | 1.96 | 29.64 | 1.70 | 0.79 | |
| Max | 12.00 | 2.50 | 81.49 | 1.84 | 1.10 | |
| P – value | 0.000 | 0.000 | 0.575 | 0.000 | 0.000 | |
Fractional shortening (FS) showed no significant difference among stages (p = 0.575).
Both LVIDd and LVIDs increased significantly across stages (p < 0.001).
3.5. NT-proBNP quantification across disease stages
NT-proBNP concentrations increased significantly with disease progression (p < 0.001) (Table 4).
Table 4. NT-proBNP concentrations in different disease stages
| Stage | Statistical parameters | Indices (NT-proBNP) |
|---|---|---|
| B1 | n | 6 |
| Mean | 500c | |
| SD | 0.00 | |
| Min | 500 | |
| Max | 500 | |
| B2 | n | 55 |
| Mean | 953.8b | |
| SD | 294.0 | |
| Min | 500 | |
| Max | 1356.2 | |
| C | n | 23 |
| Mean | 2131.8a | |
| SD | 354.4 | |
| Min | 1625.5 | |
| Max | 2935.2 | |
| P – value | 0.000 | |
Mean NT-proBNP values were 500 pg/mL (B1), 953.8 ± 294.0 pg/mL (B2), and 2,131.8 ± 354.4 pg/mL (C).
3.6. Treatment outcomes of MMVD according to disease stage
Treatment outcomes are summarised in Table 5.
Table 5. Treatment outcomes of MMVD by disease stage
| Stage | B1 | B2 | C | Total |
|---|---|---|---|---|
| Number of cases with effective treatment | 6 | 54 | 10 | 70 |
| Treatment success rate (%) | 100 | 98.18 | 43.48 | 83.33 |
| Number of cases with ineffective treatment | 0 | 1 | 13 | 14 |
| Treatment failure rate (%) | 0 | 1.82 | 56.52 | 16.67 |
In stage B2, the treatment success rate was 98.18%, with 1 case (1.82%) showing no response. In stage C, treatment success was 43.48%, whereas 56.52% of cases were non-responsive. At stage B1, no specific cardiac treatment was administered; therefore, treatment outcomes were not evaluated for this stage.
4.0 Discussion
This study evaluated the prevalence, clinical characteristics, selected diagnostic indicators, and treatment outcomes of MMVD in dogs presented to a veterinary hospital in Vietnam. Among 3,840 examined dogs, 232 (6.04%) were suspected of cardiac disease based on clinical findings, and 84 dogs were definitively diagnosed with MMVD by echocardiography, representing 36.21% of suspected cases and 2.19% of all examined dogs. These findings support the importance of echocardiography in confirming MMVD among dogs initially suspected on the basis of nonspecific clinical signs. In routine practice, heart murmur, coughing, and exercise intolerance may raise suspicion of MMVD, but these findings alone are insufficient to establish a definitive diagnosis because they may overlap with respiratory and other systemic disorders.
The clinical manifestations observed in this study were generally consistent with the expected progression of MMVD across ACVIM stages. Dogs in stage B1 showed minimal clinical abnormalities, whereas dogs in stages B2 and C showed increasingly frequent respiratory and systemic signs. Dyspnea/pulmonary oedema and cough/respiratory inflammation were the most common signs overall, and their frequency increased with disease severity. This pattern is pathophysiologically plausible, as chronic mitral regurgitation leads to progressive left atrial enlargement and elevated pulmonary venous pressure, which may result in pulmonary congestion and oedema. The marked increase in syncope frequency in stage C also reflects the hemodynamic consequences of advanced disease, including reduced forward cardiac output and impaired tissue perfusion. However, clinical signs should always be interpreted cautiously, because they are not specific for MMVD and may be influenced by concurrent respiratory disease, especially in small-breed and older dogs.
Cardiac murmur intensity also increased with disease stage in the present study. Mild murmurs predominated in stage B1, whereas grade III/VI murmurs were most common in stage B2 and more severe murmurs were more frequently observed in stage C. This finding is consistent with the clinical course of MMVD, in which progressive valvular degeneration and worsening mitral regurgitation generate a more prominent systolic murmur. Previous studies have similarly shown that murmur intensity is associated with the severity of mitral regurgitation and may help identify dogs requiring further diagnostic evaluation. Nevertheless, murmur grade should not be considered a surrogate for disease stage in all cases. Some dogs in stage C still had grade III/VI murmurs, which may be explained by factors such as thoracic conformation, pulmonary crackles, reduced cardiac output, or variation in the audibility of turbulent regurgitant flow. Therefore, although auscultation remains a valuable screening tool, staging of MMVD should rely on integrated clinical and imaging findings rather than murmur intensity alone.
Radiographic and echocardiographic findings in this study clearly reflected disease progression. Vertebral heart size, LA/Ao ratio, LVIDd, and LVIDs all increased significantly from stage B1 to stages B2 and C, indicating progressive chamber enlargement and cardiac remodelling associated with chronic volume overload. In particular, the increase in LA/Ao from 1.38 in stage B1 to 1.76 in stage B2 and 2.18 in stage C is clinically relevant, because left atrial enlargement is one of the most important indicators of disease progression and risk of developing congestive heart failure. Likewise, the increase in VHS and left ventricular internal dimensions supports the value of both thoracic radiography and echocardiography in the evaluation of MMVD severity.
The present findings are in agreement with previous reports showing that indices of left-sided volume overload are highly informative in dogs with MMVD. Boswood et al. (2016) used left atrial enlargement and increased ventricular dimensions as key criteria to identify stage B2 dogs likely to benefit from early intervention, while other studies have shown that progressive increases in VHS and chamber size are associated with worsening clinical status and poorer outcome. In contrast, fractional shortening did not differ significantly among disease stages in this study. This observation is not unexpected, because MMVD is primarily a disease of volume overload rather than primary systolic myocardial failure. In such patients, systolic indices such as FS may remain within normal or even apparently increased ranges despite substantial structural remodelling. Therefore, the lack of a significant difference in FS does not imply absence of disease progression; rather, it underscores the greater clinical value of structural measurements such as LA/Ao, LVIDd, LVIDs, and VHS in monitoring MMVD.
NT-proBNP concentrations increased markedly with disease progression, from 500 pg/mL in stage B1 to 953.8 ± 294.0 pg/mL in stage B2 and 2,131.8 ± 354.4 pg/mL in stage C. These findings support the utility of NT-proBNP as a biomarker of myocardial wall stress and progressive cardiac remodelling in dogs with MMVD. The increase observed in stage B2 is especially important, because these dogs may not yet show overt signs of congestive heart failure despite already having significant cardiac enlargement. In this context, NT-proBNP may provide additional support for risk stratification, particularly when interpreted together with echocardiographic findings. The markedly higher values observed in stage C are also consistent with overt decompensation and increased hemodynamic burden. Previous studies have similarly demonstrated that NT-proBNP is useful for distinguishing dogs with cardiac from non-cardiac causes of respiratory signs and for assessing disease severity in MMVD. Thus, the present results reinforce the role of NT-proBNP as a complementary tool, rather than a standalone test, in the diagnosis and monitoring of this disease.
Treatment outcomes differed substantially between disease stages. Dogs in stage B2 had a very high treatment success rate, whereas the response rate in stage C was much lower. This result is clinically meaningful and is consistent with the concept that earlier detection and intervention are associated with better disease control. Stage B2 dogs generally still retain effective compensatory mechanisms despite structural cardiac remodelling and therefore may respond favourably to appropriate treatment and monitoring. In contrast, dogs in stage C have already developed clinical heart failure, and treatment becomes more challenging because of greater hemodynamic instability, pulmonary oedema, and possible concurrent complications. These findings emphasize the importance of recognizing MMVD before overt decompensation occurs. They also support the current clinical approach of close monitoring and timely therapeutic intervention in dogs with evidence of cardiac enlargement even in the absence of advanced heart failure.
From a practical perspective, this study highlights the importance of combining physical examination, thoracic radiography, echocardiography, and NT-proBNP testing when evaluating dogs suspected of MMVD. No single parameter alone was sufficient to characterize disease severity across all stages. Clinical signs and murmur intensity were useful for initial screening, but imaging and biomarker evaluation provided the strongest information for staging and monitoring. In a clinical setting such as Vietnam, where access to advanced diagnostic tools may vary among facilities, these findings may help support a more structured diagnostic approach and encourage earlier identification of dogs at risk of progression.
Limitations
This study has several limitations. First, the number of dogs definitively diagnosed with MMVD was relatively limited, which may reduce the generalizability of the findings. Second, the number of dogs in the more advanced stages was relatively small, and no dogs in stage D were included, limiting assessment of the full spectrum of disease severity. Third, only a limited number of echocardiographic variables were evaluated. Additional parameters with known pathophysiological and prognostic importance, such as left atrial volume and peak E-wave velocity, were not assessed. Fourth, survival analysis was not performed, and therefore the natural history of MMVD and the long-term effects of different variables and treatment protocols could not be explored. Fifth, electrocardiographic findings were not included, and no data were available regarding arrhythmias or the use of antiarrhythmic drugs, despite the clinical relevance of rhythm disturbances in dogs with MMVD. Sixth, other cardiovascular complications, such as pulmonary hypertension and left atrial rupture, were not evaluated. Finally, information on comorbidities, particularly renal disease and tracheobronchial collapse, was not systematically collected, although such conditions may substantially influence clinical presentation, treatment response, and survival. Future studies with larger sample sizes, broader cardiovascular assessment, and long-term follow-up are needed to better define the clinical course and prognostic factors of MMVD in dogs under local practice conditions.
5.0 Conclusion
In this study, MMVD was confirmed in 2.19% of examined dogs, with prevalence increasing among those presenting with respiratory signs. Clinical signs and cardiac murmur intensity increased with disease progression, while echocardiographic variables of left-sided volume overload and NT-proBNP concentrations showed significant changes across stages.
These findings highlight the importance of combining clinical examination, diagnostic imaging, and biomarker assessment for accurate staging and monitoring of MMVD, thereby supporting earlier detection and more effective disease management in dogs.
Author Contributions: Conceptualisation: Thuy Hoang Nguyen, Quynh Ngoc Nhu Nguyen, Loan Vu Thuy Hong Nguyen; Methodology: Thuy Hoang Nguyen, Kinh Van La, Yen Hai Vu; Validation: Kinh Van La, Loan Vu Thuy Hong Nguyen; Formal analysis: Thuy Hoang Nguyen, Quynh Ngoc Nhu Nguyen, Yen Hai Vu; Investigation: Thuy Hoang Nguyen, Quynh Ngoc Nhu Nguyen; Data Curation: Quynh Ngoc Nhu Nguyen, Loan Vu Thuy Hong Nguyen; Writing—Original Draft Preparation: Thuy Hoang Nguyen, Quynh Ngoc Nhu Nguyen, Yen Hai Vu; Writing—Review and Editing: Kinh Van La, Loan Vu Thuy Hong Nguyen. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Data Availability Statement: All the relevant data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments: The authors sincerely thank Procare Veterinary Hospital for providing the clinical cases presented in this report.
Conflicts of Interest: The authors declare no conflicts of interest.
Artificial Intelligence: AI was not used for this original research article.
References
Boswood A, Häggström J, Gordon SG, Wess G, Stepien RL, Oyama MA, Keene BW, Bonagura J, MacDonald KA, Patteson M, Smith S, Fox PR, Sanderson K, Woolley R, Szatmári V, Menaut P, Church WM, O’Sullivan ML, Jaudon JP, Kresken JG, … Watson P. 2016. Effect of pimobendan in dogs with preclinical myxomatous mitral valve disease and cardiomegaly: The EPIC study – A randomized clinical trial. Journal of Veterinary Internal Medicine, 30(6), 1765–1779. https://doi.org/10.1111/jvim.14586
Borgarelli M, Crosara S, Lamb K, Savarino P, La Rosa G, Tarducci A, Haggstrom J. 2012. Survival characteristics and prognostic variables of dogs with preclinical chronic degenerative mitral valve disease attributable to myxomatous degeneration. Journal of Veterinary Internal Medicine, 26(1), 69–75. https://doi.org/10.1111/j.1939-1676.2011.00860.x
Borgarelli M, Buchanan JW. 2012. Historical review, epidemiology and natural history of degenerative mitral valve disease. Journal of Veterinary Cardiology, 14(1), 93–101. https://doi.org/10.1016/j.jvc.2012.01.011
Buchanan JW, Bücheler J. 1995. Vertebral scale system to measure canine heart size in radiographs. Journal of the American Veterinary Medical Association, 206(2), 194–199.
Cornell CC, Kittleson MD, Della Torre P, Häggström J, Lombard CW, Pedersen HD, Vollmar A, Wey A. 2004. Allometric scaling of M-mode cardiac measurements in normal adult dogs. Journal of Veterinary Internal Medicine, 18(3), 311–321. https://doi.org/10.1892/0891-6640(2004)18<311:asomcm>2.0.co;2
Fox PR. 2012. Pathology of myxomatous mitral valve disease in the dog. Journal of Veterinary Cardiology, 14(1), 103–126. https://doi.org/10.1016/j.jvc.2012.02.001
Goutal CM, Keir I, Kenney S, Rush JE, Freeman LM. 2010. Evaluation of acute congestive heart failure in dogs and cats: 145 cases (2007-2008). Journal of Veterinary Emergency and Critical Care, 20(3), 330–337. https://doi.org/10.1111/j.1476-4431.2010.00524.x
Keene BW, Atkins CE, Bonagura JD, Fox PR, Häggström J, Fuentes VL, Oyama MA, Rush JE, Stepien R, Uechi M. 2019. ACVIM Consensus Guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. Journal of Veterinary Internal Medicine, 33(3), 1127–1140. https://doi.org/10.1111/jvim.15488
Lam MC, Lin CH, Lo PY, Wu HD. 2022. Influence of concurrent lower respiratory tract disease on point-of-care lung ultrasound in small-breed dogs with myxomatous mitral valve disease. Journal of Veterinary Internal Medicine, 36(3), 1075–1081. https://doi.org/10.1111/jvim.16428
Levicar C, Nolte I, Granados-Soler JL, Freise F, Raue JF, Bach JP. 2022. Methods of radiographic measurements of heart and left atrial size in dogs with and without myxomatous mitral valve disease: Intra- and interobserver agreement and practicability of different methods. Animals, 12(19), 2531. https://doi.org/10.3390/ani12192531
Menciotti G, Borgarelli M. 2017. Review of diagnostic and therapeutic approach to canine myxomatous mitral valve disease. Veterinary Sciences, 4(4), 47. https://doi.org/10.3390/vetsci4040047
Oyama MA, Rush JE, Rozanski EA, Fox PR, Reynolds CA, Gordon SG, Bulmer BJ. Lefbom BK, Brown BA, Lehmkuhl LB, Prosek R, Lesser MB, Kraus MS, Bossbaly MJ, Rapoport GS, Boileau JS. 2009. Assessment of serum N-terminal pro-B-type natriuretic peptide concentration for differentiation of congestive heart failure from primary respiratory tract disease as the cause of respiratory signs in dogs. Journal of the American Veterinary Medical Association, 235(11), 1319–1325. https://doi.org/10.2460/javma.235.11.1319
Pedersen HD, Lorentzen KA, Kristensen BO. 1999. Echocardiographic mitral valve prolapse in Cavalier King Charles Spaniels: Epidemiology and prognostic significance for regurgitation. The Veterinary Record, 144(12), 315–320. https://doi.org/10.1136/vr.144.12.315
Pedersen HD, Häggström J, Falk T, Mow T, Olsen LH, Iversen L, Jensen AL. 1999. Auscultation in mild mitral regurgitation in dogs: Observer variation, effects of physical maneuvers, and agreement with color doppler echocardiography and phonocardiography. Journal of Veterinary Internal medicine, 13(1), 56–64.
Turgut K, Naseri A, Ince ME, Süleymanoğlu H, Ertan M, Sağmanlıgil V, Sen I. 2019. Clinical and cardiologic assessment of Anatolian shepherd dogs with asymptomatic degenerative mitral valve disease. International Journal of Advanced and Applied Sciences, 6(7), 29–35. https://doi.org/10.21833/ijaas.2019.07.004
van Staveren MDB, Muis E, Szatmári V. 2023. Self-reported utilization of international guidelines for staging dogs with myxomatous mitral valve degeneration: A survey among veterinary practitioners. Veterinary Sciences, 10(12), 687. https://doi.org/10.3390/vetsci10120687
Disclaimer/Publisher’s Note: The statements, opinions, institutional affiliations, data contained in all publications, and all responsibilities for accuracy are solely those of the individual author(s) and contributor(s) and not of MARCIAS AUSTRALIA and AJAVAS/or the Editor(s). MARCIAS AUSTRALIA and AJAVAS/or the Editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.